Conditions with Underlying T2I
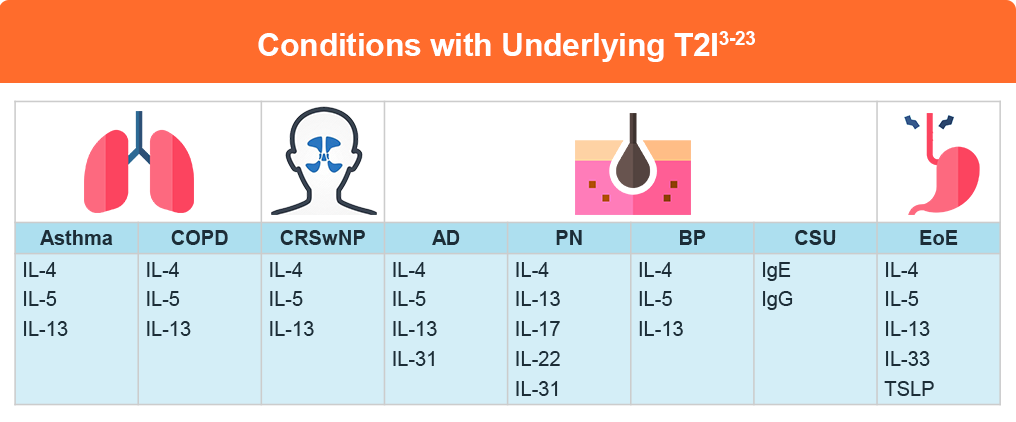
Type 2 inflammation (T2I) plays a crucial role in several allergic and inflammatory diseases, including asthma, atopic dermatitis (AD), chronic rhinosinusitis with nasal polyps (CRSwNP), eosinophilic esophagitis (EoE), prurigo nodularis (PN), bullous pemphigoid (BP), chronic spontaneous urticaria (CSU), and chronic obstructive pulmonary disease (COPD).1
Comorbid presentation of type 2 inflammatory diseases is common and is associated with a greater clinical and quality-of-life burden. Patients should be assessed for comorbid diseases.2 Better understanding the contribution of T2I to these diseases is critical to providing a patient-centered approach to diagnosis and individualized treatment and, thus, to improving patient outcomes.
Asthma
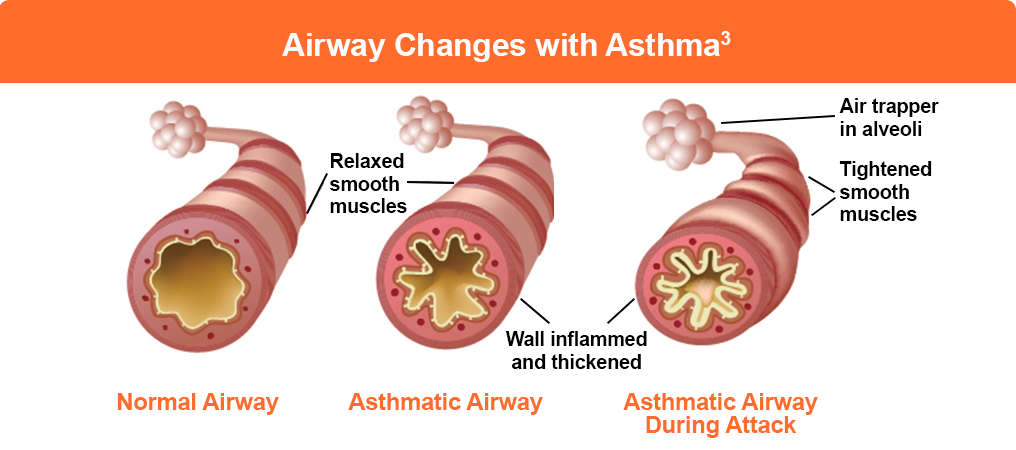
Asthma represents the most studied type 2 inflammatory disease, with roughly 84% of asthma patients exhibiting T2I characterized by increased blood or sputum eosinophils whose counts correlate with disease severity.4 Infiltrating tissue eosinophils are a source of potent type 2 proinflammatory signals (including type 2 cytokines IL-4, IL-5 and IL-13) that facilitate lung tissue remodeling leading to airway thickening and fibrosis. Impaired lung function over time further leads to exacerbations and poor asthma control, highlighting the importance of early identification for optimal control.5,6
Atopic Dermatitis

Atopic dermatitis (AD) is a common, chronic, inflammatory skin disease characterized by intense itch, recurring eczematous skin lesions, and greatly reduced quality of life for patients and their caregivers. Type 2 inflammation plays a significant role in AD pathophysiology, with key type 2 cytokines implicated including IL- 4, IL-5, IL-13 and IL-31.9
T2I leads to multiple clinical features associated with eczematous lesions, including intense itch, barrier dysfunction, and increased risk of skin infections. Up to 80% of atopic dermatitis patients present with other type 2 inflammatory diseases.1
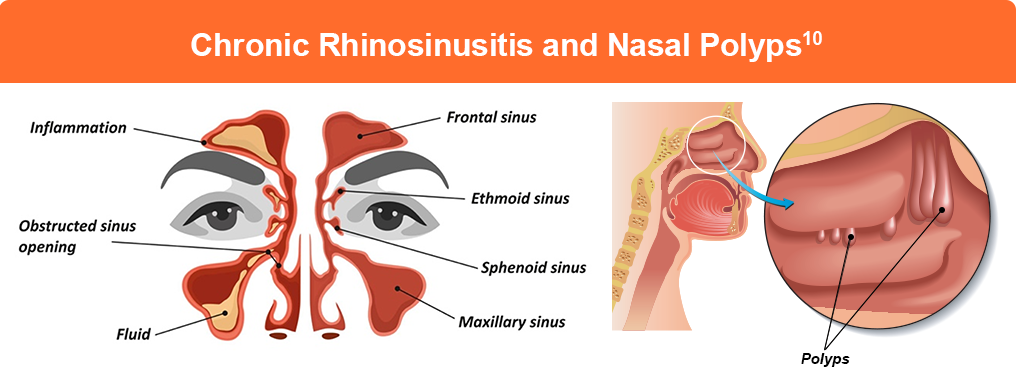
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a chronic inflammatory disease marked by grape-like projections of inflammatory polyps within the nasal cavity leading to a myriad of persistent symptoms including nasal congestion, post-nasal drip, facial pressure or pain, rhinorrhea, and loss of smell, all of which negatively affect the patient’s health-related quality of life.11-13 Asthma commonly co-occurs with CRSwNP, and symptoms for both diseases are often exacerbated in these patients.14
Approximately 80% of CRwNP cases present with T2I characterized by an increase in IL-4, IL-5, and IL-13 production by TH2 and ILC2 cells.15-18
Chronic Obstructive Pulmonary Disease
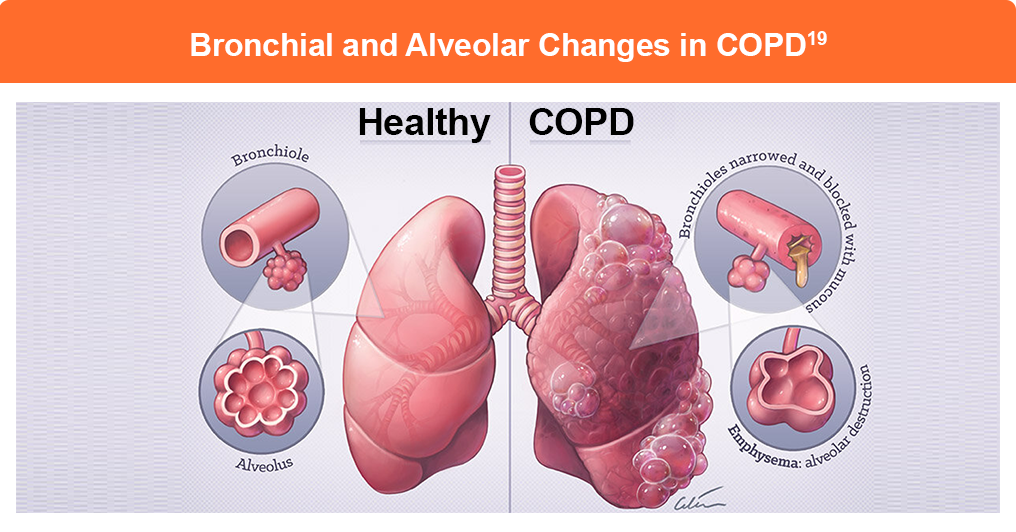
T2I is present in up to 40% of patients with COPD and is associated with an increased risk of exacerbations.20 Cytokines commonly elevated in these patients include IL-4, IL-5, IL-13, with ILC2 and TH2 cells also elevated. These changes can cause raised eosinophil counts in sputum, bronchial tissue, and blood, and/or elevated levels of fractional exhaled nitric oxide.21
Eosinophilic Esophagitis
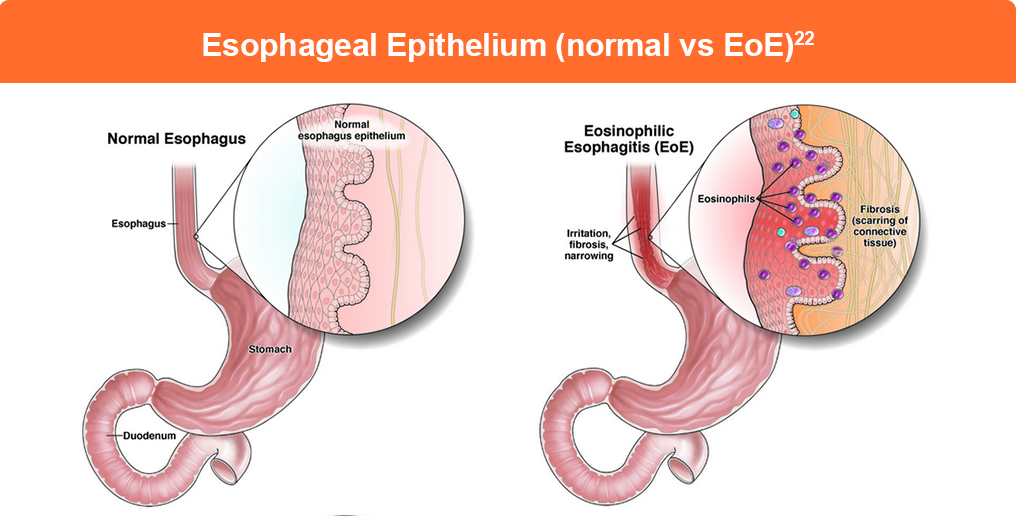
Eosinophilic esophagitis is a chronic, allergen-driven, type 2 inflammatory disease of the esophagus. Persistent T2I in untreated EoE leads to stricture formation, magnifying the clinical sequelae of dysphagia, food impactions, and a markedly diminished quality of life.23 A dysregulated feed-forward cycle that develops between an abnormal esophageal epithelium and the immune system is central to EoE pathophysiology. The esophageal epithelium with impaired barrier function stimulates allergen-induced type 2-biased immune activation. Characteristic Th2 cytokines include interleukin IL-33, TSLP, IL-4, IL-5, and IL-13.24
Prurigo Nodularis
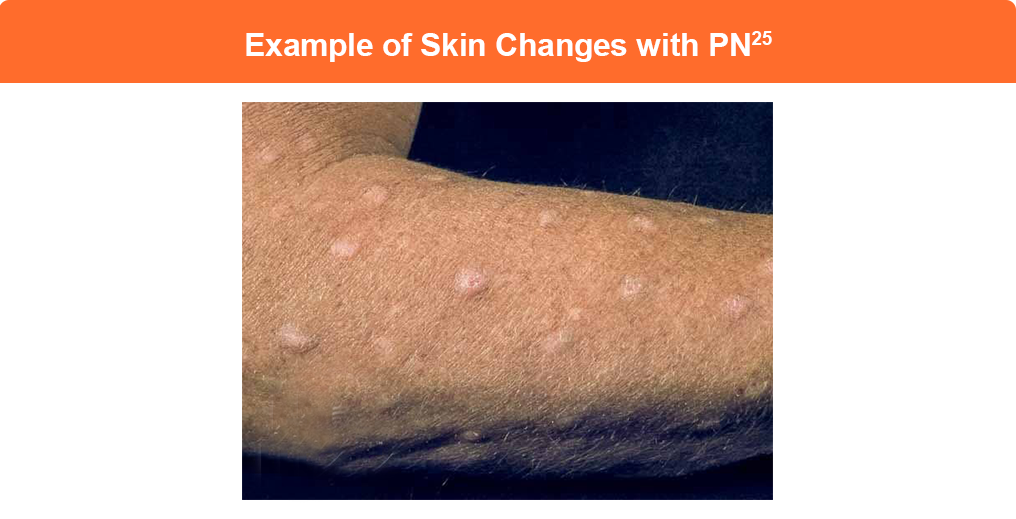
Prurigo nodularis (PN) is a highly burdensome condition that presents with pruritic nodules on the skin of extremities and the trunk and is characterized by an intractable itch-scratch cycle, severely impacting patient quality of life. Its pathogenesis is associated with immune dysregulation mediated by cytokines, including IL-4, IL-13, IL-17, IL-22 and IL-31, indicating a role for type 2 inflammation alongside Th17 and Th22-mediated inflammation.26
Bullous Pemphigoid

Bullous pemphigoid (BP) is an autoimmune blistering disease that mainly occurs in the elderly. T2I plays a central role in the pathogenesis of BP, beginning when autoantibodies target two proteins in the skin’s basement membrane zone: BP180 and BP230. This activates Th2 cells and ILC2s, which produce inflammatory cytokines including IL-4, IL-5, and IL-13.27,28
IL-4 promotes Th2 cell differentiation and drives B cells to produce IgE antibodies—a hallmark of BP found in 70%-85% of patients. IL-5 supports eosinophil development and survival, explaining why eosinophilia is common in BP and correlates with disease severity. IL-13 works synergistically with IL-4 to enhance IgE production and is associated with itch severity. The presence of elevated IgE leads to mast cell and basophil activation, causing the release of inflammatory mediators that contribute to tissue damage and blister formation.27,28
Chronic Spontaneous Urticaria

Chronic spontaneous urticaria (CSU) is an autoimmune condition characterized by the recurrent appearance of itchy wheals and/or angioedema that persists for several months or years. There are two main types:31,32
- Type I autoimmune CSU involves IgE autoantibodies against self-antigens like thyroid peroxidase (TPO) and IL-24. This “autoallergic” form is characterized by elevated total IgE levels and often responds well to anti-IgE therapies
- Type IIb autoimmune CSU involves IgG autoantibodies that activate mast cells, particularly antibodies against the high-affinity IgE receptor (FcεRI) or IgE itself. This form affects less than 10% of CSU patients when strict diagnostic criteria are used. It is associated with more severe disease, concurrent autoimmune conditions, low total IgE levels, reduced blood basophils and eosinophils, and poorer response to antihistamines and biologics. Some patients show evidence of both types.
References
- Ogulur I, Mitamura Y, Yazici D, Pat Y, Ardicli S, Li M, D’Avino P, Beha C, Babayev H, Zhao B, Zeyneloglu C, Giannelli Viscardi O, Ardicli O, Kiykim A, Garcia-Sanchez A, Lopez JF, Shi LL, Yang M, Schneider SR, Skolnick S, Dhir R, Radzikowska U, Kulkarni AJ, Imam MB, Veen WV, Sokolowska M, Martin-Fontecha M, Palomares O, Nadeau KC, Akdis M, Akdis CA. Type 2 immunity in allergic diseases. Cell Mol Immunol. 2025 Mar;22(3):211-242.
- Gómez de la Fuente E, Alobid I, Ojanguren I, et al. Addressing the unmet needs in patients with type 2 inflammatory diseases: when quality of life can make a difference. Front Allergy. 2023;4:1296894.
- Lynn SJ, Kushto-Reese K. Understanding asthma pathophysiology, diagnosis and management. My American Nurse. July 7, 2015. https://www.myamericannurse.com/understanding-asthma-pathophysiology/
- Jackson D, Aljamil N, Roxas C, et al. P48 The ‘T2-low’ asthma phenotype: Could it just be T2-high asthma treated with corticosteroids? Thorax. 2018;73(suppl 4):A124-A125.
- Haselkorn T, Fish JE, Zeiger RS, et al. Consistently very poorly controlled asthma, as defined by the impairment domain of the Expert Panel Report 3 guidelines, increases risk for future severe asthma exacerbations in The Epidemiology and Natural History of Asthma: Outcomes and Treatment Regimens (TENOR) study. J Allergy Clin Immunol. 2009;124(5):895-902.e1-4.
- Patel M, Pilcher J, Reddel HK, et al. Predictors of severe exacerbations, poor asthma control, and β-agonist overuse for patients with asthma. J Allergy Clin Immunol Pract. 2014;2:751-758.
- Atopic dermatitis. Shutterstock. https://www.shutterstock.com/image-photo/pattern-atopic-eczema-fungal-diseases-on-2180479667
- Atopic dermatitis. Shutterstock. https://www.shutterstock.com/image-photo/atopic-dermatitis-on-folds-hands-731756785
- Beck LA, Cork MJ, Amagai M, et al. Type 2 inflammation contributes to skin barrier dysfunction in atopic dermatitis. JID Innov. 2022;2:100131.
- Asthma and Allergy Network. What is chronic rhinosinusitis with nasal polyps CRSwNP)? https://allergyasthmanetwork.org/health-a-z/chronic-rhinosinusitis-with-nasal-polyps-crswnp/
- Chen S, Zhou A, Emmanuel B, Thomas K, Guiang H. Systematic literature review of the epidemiology and clinical burden of chronic rhinosinusitis with nasal polyposis. Curr Med Res Opin. 2020;36:1897-1911.
- Bachert C, Han JK, Wagenmann M, et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: Definitions and management. J Allergy Clin Immunol. 2021;147:29-36.
- Morse JC, Miller C, Senior B. Management of chronic rhinosinusitis with nasal polyposis in the era of biologics. J Asthma Allergy. 2021;14:873-882.
- Langdon C, Mullol J. Nasal polyps in patients with asthma: Prevalence, impact, and management challenges. J Asthma Allergy. 2016;9:45-53.
- Bachert C, Akdis CA. Phenotypes and emerging endotypes of chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2016;4:621-628.
- Smith KA, Pulsipher A, Gabrielsen DA, Alt JA. Biologics in chronic rhinosinusitis: An update and thoughts for future directions. Am J Rhinol Allergy. 2018;32:412-423.
- Maniu AA, Perde-Schrepler MI, Tatomir CB, et al. Latest advances in chronic rhinosinusitis with nasal polyps endotyping and biomarkers, and their significance for daily practice. Rom J Morphol Embryol. 2020;61:309-320.
- Zhai Z, Shao L, Lu Z, et al. Characteristics of mucin hypersecretion in different inflammatory patterns based on endotypes of chronic rhinosinusitis. Clin Transl Allergy. 2024;14:e12334.
- GIG CYMRU. NHS Wales. Chronic Obstructive Pulmonary Disease (COPD). https://abuhb.nhs.wales/hospitals/a-z-of-services/respiratory-medicine/chronic-obstructive-pulmonary-disease-copd/
- Varricchi G, Poto R. Towards precision medicine in COPD: Targeting type 2 cytokines and alarmins. Eur J Intern Med. 2024;125:28-31.
- Polverino F, Sin DD. Type 2 airway inflammation in COPD. Eur Respir J. 2024;63:2400150.
- AGA gi patient center. Eosinophilic esophatitis (EoE). https://patient.gastro.org/eosinophilic-esophagitis/
- Nhu QM, Aceves SS. Current state of biologics in treating eosinophilic esophagitis. Ann Allergy Asthma Immunol. 2023;130:15-20.
- Underwood B, Troutman TD, Schwartz JT. Breaking down the complex pathophysiology of eosinophilic esophagitis. Ann Allergy Asthma Immunol. 2023;130:28-39.
- DermNet®. Nodular prurigo. https://dermnetnz.org/topics/nodular-prurigo
- Liao V, Cornman HL, Ma E, Kwatra SG. Prurigo nodularis: New insights into pathogenesis and novel therapeutics. Br J Dermatol. 2024;190:798-810.
- Zhang L, Chen Z, Wang L, Luo X. Bullous pemphigoid: The role of type 2 inflammation in its pathogenesis and the prospect of targeted therapy. Front Immunol. 2023;14:1115083.
- Toh WH, Lee HE, Chen CB. Targeting type 2 inflammation in bullous pemphigoid: Current and emerging therapeutic approaches. Front Med (Lausanne). 2023;10:1196946.
- English dermatology. Bullous Pemphigoid. https://www.englishdermatology.com/services/bullous-pemphigoid/
- Kocatürk E, Chu DK, Turk, M et al. Management of Chronic Spontaneous Urticaria Made Practical: What Every Clinician Should Know. J Allergy Clin Immunol Pract. 2025;13(9): 2252-2269
- Sella JA, Ferriani MPL, Melo JML, et al. Type I and type IIb autoimmune chronic spontaneous urticaria: Using common clinical tools for endotyping patients with CSU. J Allergy Clin Immunol Glob. 2023;2:100159.
- Kolkhir P, Muñoz M, Asero R, et al. Autoimmune chronic spontaneous urticaria. J Allergy Clin Immunol. 2022;149:1819-1831.
All URLs accessed January 23, 2025
